A dental x-ray and cone-beam computed tomography (CBCT) imaging aided in diagnosing and treating a 20-year-old man's bilateral kissing molars, an extremely rare form of impaction. The case report was published on November 12 in the Clinical Case Reports.
The report is one of nine similar cases reported in the literature. Therefore, there is limited guidance outlining the management of kissing molars, which is when the occlusal surfaces of these impacted teeth are connected by the same follicular space and their roots point in the opposite direction, the authors wrote.
"Very few bilateral cases have been published in the literature, so this case adds to this small cohort with the hope to increase awareness and ultimately optimize confidence for onward referral and management," wrote the authors, led by Emma Carr of Queen Elizabeth Hospital in Glasgow, U.K.
A 20-year-old man with a dull ache
In August 2011, the patient, who had a dull ache in the left angle of the jaw for 12 months, was referred from his general dentist to an oral and maxillofacial surgeon. The man was healthy but smoked 10 cigarettes per day for two years and drank about 14 alcoholic drinks per week.
An exam revealed no facial asymmetry, significant extraoral findings, or soft-tissue abnormalities. The following seven teeth had not erupted:
- Upper right tooth #7 and #8 (based on the Palmer tooth numbering system)
- Upper left tooth #8
- Lower left tooth #7 and #8
- Lower right tooth #7 and #8
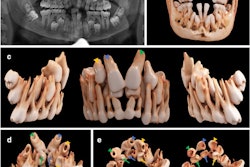
Additionally, the man's upper left second premolar was missing. A panoramic x-ray revealed bilateral kissing molars in his lower quadrants linked with cystic lesions encompassing the molar crowns. Also, it was noted that an ectopic upper right #8 tooth accompanied an associated mass in the right maxillary antrum. To determine the risks of surgically removing these teeth, the man was told to get a CBCT scan, the authors of the case report wrote.
 A panoramic x-ray revealed the patient's bilateral kissing molars. Image courtesy of Carr et al. Licensed by CC BY 4.0.
A panoramic x-ray revealed the patient's bilateral kissing molars. Image courtesy of Carr et al. Licensed by CC BY 4.0.The CBCT revealed the following features:
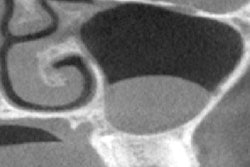
- A 17 mm vertical x 18 mm mediolateral x 24 mm anterior-posterior corticated soft-tissue mass in the right maxillary sinus, which was intimately involved with the displaced upper right tooth #8
- Thinning of the right maxillary sinus wall with a vertical dimension in excess of 28 mm and a mass involving the crowns of the upper right teeth #8 and #7
- The apices of the upper right tooth #8 were dilacerated and engaged the lateral wall of the right maxillary sinus
- The roots of the upper right tooth #7 engaged the floor of the maxillary sinus and the floor of the right nasal cavity, and the tooth's root was situated between the roots of the upper right #6 tooth
- The upper right tooth #6 had apical root resorption of the distobuccal root, blunting its palatal root
- The upper right tooth #5 was two rooted
- The upper left tooth #8 had dilacerated roots and engaged the floor of the left maxillary sinus
- The upper left tooth #4 was rotated
- The lower right teeth #6 and #7 showed a kissing molar arrangement with follicular expansion that measured up to 5 mm
- The roots of lower right tooth #7 displaced the right canal lingually
- Lower left teeth #7 and #8 showed a kissing molar arrangement with follicular expansion in a similar pattern to the contralateral side
- The right canal followed a lingual course through the mandible's ramus and ran lateral to and inferior to the expanded follicle before being displaced lingually by the crown and root structure of the lower right tooth #7
- The left canal followed a lingual course through the mandible's ramus before it was displaced interior by the follicle of the kissing molar, which then swung lingually, directly contacting with the roots of the lower left tooth #7 before rounding the apices to emerge as the left mental foramen
- The apices of lower left tooth #7 and lower right tooth #7 projected to the mental foramen
The man underwent a biopsy of the lesion in the lower left quadrant, and lab tests confirmed it was a dentigerous cyst. After discussions with an oral and maxillofacial consultant, the patient agreed to have the upper right teeth #7 and #8 and the lower kissing molars extracted due to the risk of damage to the inferior alveolar nerves. The man underwent the procedure and was given analgesics and a chlorhexidine rinse and had a successful recovery, according to the report.
 Clinical images taken during surgical removal of the patient's kissing molars.
Clinical images taken during surgical removal of the patient's kissing molars.At a three-month visit, the soft tissue had healed completely, and the patient reported no other symptoms, the authors wrote.
Understanding kissing molars
The etiology of kissing molars remains unknown. There are theories that an ectopic tooth bud may be the cause and that early cystic development around a molar may cause crowns to displace, they wrote.
In some cases, there is a high risk of pathological fracture and inferior alveolar nerve injury. Deflection of the roots, narrowing of the roots, diversion of the canal, and narrowing of the canal are features found on imaging that would suggest a high risk of inferior alveolar nerve damage. In such cases, a CBCT scan can provide beneficial information about the buccolingual positioning of the inferior alveolar nerve and the width of the remaining bone, which aids in treatment planning, the authors wrote.
"Despite continuing research being needed to determine the etiology of this phenomenon, it is hoped that this case report will raise awareness and improve understanding of kissing molars so that clinicians can correctly diagnose, manage, or refer patients as appropriate," Carr and colleagues wrote.