You just placed a restoration and have a choice -- do you use silver diamine fluoride (SDF), reducing the risk of secondary caries but also staining the tooth, or do you leave it as is? New research suggests SDF with potassium iodide might be a compromise between the two options.
Silver diamine fluoride with potassium iodide (SDF+KI) reduced secondary caries while also minimizing the amount of staining around a restoration, according to a recent study in the International Journal of Molecular Sciences (February 6, 2017). While the combination treatment may not work as well as SDF alone, it could be a balance between a perfect aesthetic and caries recurrence.
"SDF+KI treatment inhibited development of secondary caries on [glass ionomer composite] restorations, but was not as effective as SDF treatment alone," wrote the authors, led by Irene Shuping Zhao, a doctoral student at the University of Hong Kong dental school. "Moreover, SDF+KI treatment caused a perceptible staining at the restoration margin, but the intensity was less than that with purely SDF treatment."
SDF+KI as a compromise
Secondary caries is the most common reason for restoration replacement, even for glass ionomer cements (GIC), which have antimicrobial properties. Although silver diamine fluoride has proved to effectively halt secondary caries development, it leaves black stains on teeth. Some researchers have suggested SDF with potassium iodide may be able to prevent secondary caries without also staining teeth, but no previous studies had investigated this idea.
“SDF+KI treatment inhibited development of secondary caries on GIC restorations, but was not as effective as SDF treatment alone.”
The researchers began their experiment by drilling identical rectangular cavities into 30 extracted upper and lower premolars. They then divided the teeth into three treatment groups:
- SDF+KI -- Silver diamine fluoride at a concentration of 38% with potassium iodide (Riva Star, SDI) as the intervention group
- SDF alone -- Silver diamine fluoride at a concentration of 38% (Saforide, Toyo Seiyaku Kasei) as a positive control
- No treatment -- Neither silver diamine fluoride nor potassium iodide as a negative control
Once each group was treated with the corresponding intervention, or lack thereof, the researchers filled the cavities with a GIC restoration (Fuji VII capsule, GC International). The restorations were then stored for 24 hours in 100% humidity.
After the first day, the researchers ran all 30 teeth through a thermocycler repeatedly for seven days to simulate the aging process. The following week, they soaked each restoration in a plate with caries-causing bacteria, including Streptococcus mutans and Actinomyces naeselundii.
At the end of the experiment, the researchers measured outer lesion depth using micro-CT and organic structures using a spectrometer. The researchers also took four color measurements throughout the process:
- Before applying the initial treatment (day 0)
- After the first 24 hours (day 1)
- After the weeklong thermocycler process (day 8)
- After soaking in bacteria for a week (day 15)
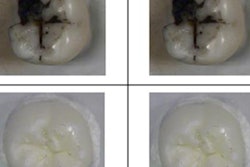
The researchers found that SDF+KI could prevent secondary caries around the GIC restorations, but not as effectively as SDF alone. However, the teeth treated with both SDF and potassium iodide were significantly less discolored than those treated with SDF alone.

"This finding might suggest KI may influence the effectiveness of SDF in preventing the formation of secondary root caries," the authors wrote. "The probable reason is that the application of KI solution might reduce the amount of silver ions."
Need for an in vivo study
Although the research evaluated a previously unstudied claim and the authors intentionally used brands easily available to practicing dentists, it was an in vitro study of only 30 molars. As such, the results may not be applicable to glass ionomer cement restorations applied in a clinical setting.
Although the authors didn't mention future study plans, they did suggest an in vivo study would be more relevant practicing dentists and urged caution when reading the results.
"It is noteworthy that this laboratory study is based on a laboratory model, which is different from the more complex clinical situation," the authors wrote. "The results cannot be extrapolated directly to the in vivo condition and caution is advised in the interpretation of the results."